

Individuals who have dizziness from cervical origin typically have several general symptoms, including neck pain, balance impairment including unsteadiness, lightheadiness and drunkeness. Types of patients with this condition range from the elderly with cervical arthritis (slow onset of symptoms) to status-post mild traumatic brain injury (mTBI) following a concussion or whiplash (fast onset of symptoms).
For the purpose of this post, we will examine the importance of cervical extensors in Cervicogenic Dizziness. Considering head extension is a primary impairment for onset of symptoms in the Cervicogenic Dizziness population, this is a significant area of interest.
The suboccipital musculature is central to promoting and resisting head motion. These motions include flexion, extension, and rotation. The suboccipital musculature associated with cervical extension are the rectus capitis posterior major (rectus capitis-PMaj), rectus capitis posterior minor (rectus capitis-PMin), and obliquees capitis inferior (OCI). Additional cervical extensors are the semispinalis cervicis, multifidus, semispinal capitis, and splenius capitis.
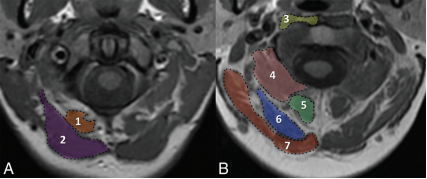
Photo courtesy of:
Fahkran et al 2016.
Previously, it has been found that atrophy of the suboccipital muscles is associated with chronic neck pain (Andary et al). In fact, greater atrophy in the rectus capitis-PMaj and rectus capitis-PMin among the suboccipital muscles have been found in patients with persistent whiplash symptoms (Elliot et al) Additionally, atrophy of these muscles has been associated with higher inflammatory biomarkers, hyperalgesia, and worse outcomes in patients with whiplash (Sterling et al)
Furthermore, rectus capitis-PMin has been associated with greater symptomatology, poorer outcome, and posttraumatic headaches after mild TBI (Fakhran et al). Additionally, atrophy of the suboccipital muscles following whiplash is involved in marked, chronic neck pain and reduced standing balance (McPartland et al).

Photo courtesy of Yuan et al 2017
Even though most research conducted with the rectus capitis-PMin correlates this muscle with the myodural bridge and association with cervical headaches, we believe there is a paucity of research analyzing this area in regards to Cervicogenic Dizziness and complex dizziness symptoms.
The rectus capitis-PMin has the greatest concentration of muscle spindles among the suboccipital musculature, which, in addition to allowing flexible movement, act as specific sensory receptors. This role is accomplished secondary to an especially high concentration of large diameter A- fibers, which convey proprioceptive information.
Even though we may not be able to prevent onset of mTBI, concussion, whiplash symptoms with strengthening the deep cervical extensors, we can certainly utilize this knowledge in our rehabilitation setting.
Or, we could even look at this at another angle and potentially utilize this knowledge in fall prevention programs to address coordinated afferent input from the cervical spine to the balance centers. As far as we know, there is some literature on manual therapies (such as Holt et al 2016 & Doughtery et al 2012) to improve balance in elderly but to our knowledge, no studies with specific deep cervical extensor strengthening. Adding this component to a multi-disciplinary approach of balance and strength training, could reduce overall risk, especially with tasks involving cervical movements.
The modern rehabilitation of Cervicogenic Dizziness is now transforming into additional sensorimotor training aspects instead of just manual therapies. The multisensory integration in neck pain and dizziness arises from multiple sources and deep cervical extensors can be highly involved in impaired on clinical examination. We include deep cervical extensor training into our Physio Blend, which helps to improve outcomes in this population.
You can learn more about the screening and treatment process of Cervicogenic Dizzinesss through Integrative Clinical Concepts, where the authors (husband–a manual therapist a wife—a vestibular specialist), teach a very unique course combining both the theory and practice of vestibular and manual principles in their 2-day course. Pertinent to this blog post, the 2nd day includes the “Physio Blend”, a multi-faceted physiotherapist approach to the management of Cervicogenic Dizziness, which includes treatments of the articular and non-articular system of manual therapy and the most updated sensorimotor exercise regimen.
If you would like to host a course for your staff (either a vestibular, neuro, sports or ortho clinic), please do not hesitate to contact me at harrisonvaughanpt@gmail.com for more information.
AUTHORS
Harrison N. Vaughan, PT, DPT, OCS, Dip. Osteopracic, FAAOMPT
Instructor: Cervicogenic Dizziness for Integrative Clinical Concepts
Danielle N. Vaughan, PT, DPT, Vestibular Specialist
Instructor: Cervicogenic Dizziness for Integrative Clinical Concepts
Want to learn in person? Attend a #manualtherapyparty! Check out our course calendar below!

Learn more online!


Want an approach that enhances your existing evaluation and treatment? No commercial model gives you THE answer. You need an approach that blends the modern with the old school. Live cases, webinars, lectures, Q&A, hundreds of techniques and more! Check out Modern Manual Therapy!
Keeping it Eclectic...













{kind=link}
Post a Comment
Post a Comment